How IOP and PHP Work Together to Ensure Long-Term Recovery and Wellness

Every individual’s path to healing is unique, requiring different levels of support and care along the way. Two critical components of a comprehensive recovery plan are Partial Hospitalization Programs (PHP) and Intensive Outpatient Programs (IOP). While each serves a distinct purpose, they often work best when combined, ensuring a seamless transition from structured care to long-term independence.
At River’s Bend, we understand that sustainable recovery requires a balance of support, structure, and personal responsibility. This guide will help you understand the key differences between PHP and IOP, how they complement each other, and when one might be the right choice for you or a loved one.
What Is a Partial Hospitalization Program (PHP)?
A Partial Hospitalization Program (PHP) is one of the highest levels of outpatient care available. It provides intensive therapy while allowing clients to return home or to a sober living environment in the evenings.
Key Features of PHP:
- Structured day-long therapy sessions, 6 hours per day, for 10–15 weekdays depending on individual needs.
- Access to medical and psychiatric support.
- Individual and group therapy.
- Holistic approaches such as mindfulness, nutrition, and stress management.
- A step-down alternative to inpatient treatment for those who still need intensive care but don’t require 24/7 supervision.
Typical PHP Day Schedule
- Morning welcome and check-in group
- Didactic Session: education
- Group Process: personal experience of a topic
- Lunch and Break
- Skills Group
- Skills Activation Group
- Check out group and goal-setting
Who Benefits Most from PHP?
- Individuals transitioning from residential/inpatient rehab
- Those needing medical and psychiatric oversight while stabilizing
- Clients requiring intensive therapy but with a supportive home environment
What Is an Intensive Outpatient Program (IOP)?
An Intensive Outpatient Program (IOP) for mental health or substance abuse provides structured support for individuals while allowing them to maintain work, school, and family commitments. It is less time-intensive than PHP but offers comprehensive therapy and relapse prevention tools. The program runs for an average of 6–8 weeks but can be individualized depending on a client’s needs. Clients can choose from daytime, afternoon, or evening, virtual or in-person. During the session, various topics are presented and discussed, allowing for group discussion facilitated by a certified therapist. At River’s Bend, IOPs are offered in specialized tracks for men, women, trauma, and grief to ensure more focused, relevant, and supportive care tailored to each client’s needs.
Key Features of IOP:
- Therapy sessions are 3 times a week, for 3 hours per session
- Focus on relapse prevention, coping strategies, and life skills
- Encourages reintegration into daily life while maintaining treatment support
Who Benefits Most from IOP?
- Individuals transitioning from PHP or inpatient rehab
- Those who need continued therapy but with more flexibility
- Clients who have established some stability but still require accountability and structure
How PHP and IOP Work Together for Long-Term Recovery
Many clients start in PHP and transition to IOP as they gain stability and independence. This gradual step-down approach ensures that they receive the support they need at each phase of recovery without feeling overwhelmed or isolated.
Benefits of Combining PHP & IOP:
- Smooth Transition: Moving from PHP to IOP helps maintain continuity of care without abrupt changes.
- Personalized Support: Treatment plans are tailored, allowing clients to receive appropriate levels of care as they progress.
- Preventing Relapse: A structured step-down process significantly reduces the risk of relapse by providing ongoing support.
- Encouraging Independence: While PHP offers intensive guidance, IOP encourages clients to apply recovery skills in real-life situations.
Many individuals seeking PHP or IOP treatment may also struggle with co-occurring mental health and substance use disorders, making integrated care essential for long-term success. At River’s Bend, we emphasize treating both addiction and mental health together to ensure a comprehensive, evidence-based recovery plan. Learn more about why treating mental health and substance use together is essential.
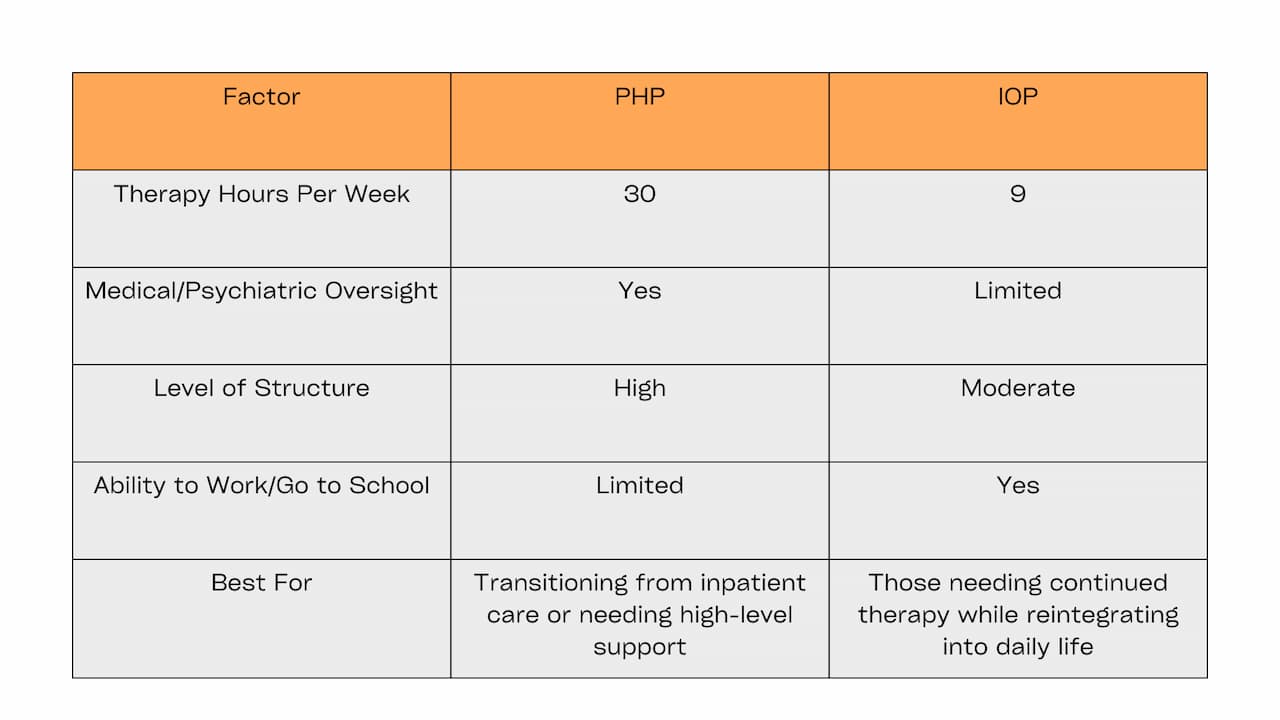
PHP vs. IOP?
It’s important to select the right level of care based on your needs, progress, and support system.
Lasting Wellness Starts at River’s Bend
Our therapists go beyond the standardized approach often found in large, corporate-run treatment centers. As a privately owned, mission-driven facility, we are dedicated to personalized, client-centered care—not a one-size-fits-all model.
What Makes River’s Bend Different?
Personalized Care Over Corporate Protocols – Unlike larger treatment facilities that follow rigid corporate structures, we have the flexibility to tailor care plans based on each client’s unique needs, progress, and goals.
- A Mission-Driven Approach – Our focus is not on numbers or quotas but on healing, transformation, and long-term success for every individual who walks through our doors.
- A Close-Knit, Compassionate Environment – Clients at River’s Bend aren’t just another case file. They become part of a supportive, nurturing community where their well-being is prioritized every step of the way.
- Seamless Transitions for Lasting Recovery – Our team works closely with each client to ensure a smooth transition from PHP to IOP and beyond, setting them up for sustainable recovery and mental wellness.
Contact River’s Bend today to schedule a consultation.
References
- Uhsinc_Remote. (2024, May 14). Understanding partial hospitalization programs | Beaumont BH. Beaumont Behavioral Hospital. https://beaumontbh.com/blog/understanding-partial-hospitalization-programs-phps/
- Lloyd‐Evans, B., & Johnson, S. (2019). Community alternatives to inpatient admissions in psychiatry. World Psychiatry, 18(1), 31–32. https://doi.org/10.1002/wps.20587
- McCarty, D., Braude, L., Lyman, D. R., Dougherty, R. H., Daniels, A. S., Ghose, S. S., & Delphin-Rittmon, M. E. (2014). Substance Abuse Intensive Outpatient Programs: Assessing the evidence. Psychiatric Services, 65(6), 718–726. https://doi.org/10.1176/appi.ps.201300249